In a recent post on Linkedin James Kennedy, public affairs director at European Society of Cardiology highlights the fact that there are more female cardiovascular deaths than male deaths in Europe.
When you compare a identical number of deaths between males and females 40% of these deaths within the female group result from a cardiovascular disease. And with males this number is only 34%.

Which is a strange phenomena since we can hardly expect females have such a different lifestyle which results in this significant difference. Another reason might be a significant physical difference between the female and the male heart and again there difference are of course real but are most probable not the major cause of this difference.
The data on plausible causes why we see more female cardiovascular deaths than male is more difficult to find in the open access database of the European Society of Cardiology.
In our perspective the base technology of diagnosing males and females on CVD should be part of the root cause analysis. And this base technology often is the 12 lead Electrocardiogram.
And this is where the gender difference comes into play. The torso positions of the pre-cordial electrodes (the 6 electrodes most close to the heart) have been defined some 70 years ago and these positions are based on male torso’s. And there’s no complementary recommendation for placing ECG electrodes on female torso’s. Placing ECG electrodes on the correct spot is something nurses and physicians are trained in. In these training sessions there’s no difference in male and female torso positions. But in real clinical life studies show in case of male ECG recordings one or more of the pre-cordial ECG electrodes are not correct placed in 50% of the cases. And in female ECG recordings this percentage is 80%. As can be expected with female ECG recording often the ECG electrodes are placed under or above the female breasts. Which has an impact on the amplitudes recorded by these electrodes.
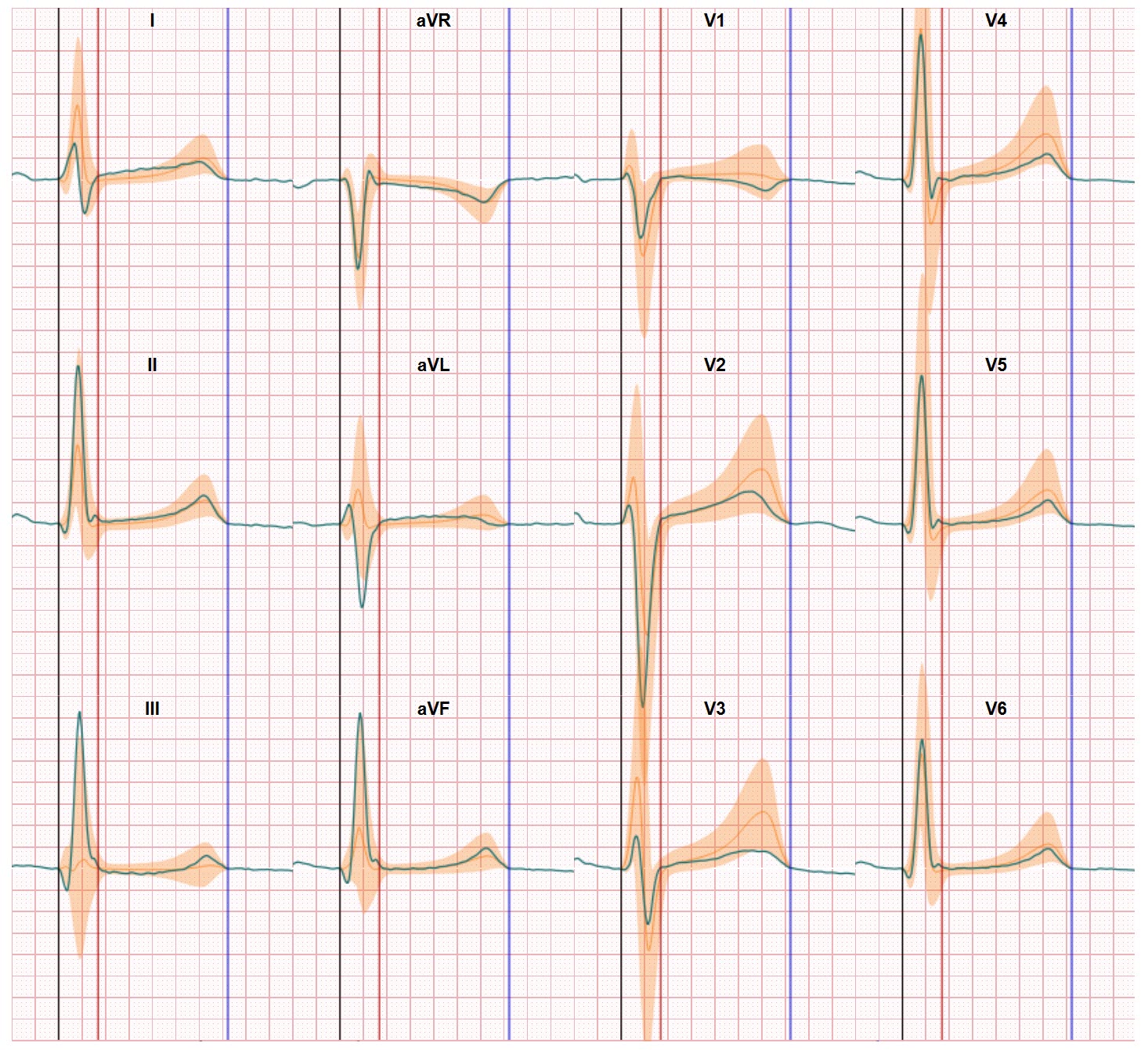
Differences between ‘normal’ male and female ECG amplitudes are clear
In our research we have found that amplitudes of normal healthy persons differ between males and females. Especially QRS and peak T-wave amplitudes are smaller in women than in men. But the differences are small and not that easy to see when one has to evaluate the graphs of a regular 12 lead ECG.

The risk of women being assessed as having a normal heart performance based on male normal is apparent and may result in a delayed detection of a cardiac disorder and thus to the phenomena of more female cardiovascular deaths than male. More on this difference can be found in the article written by Proniewska, Abächerli and van Dam in the Journal of Electrocardiology.
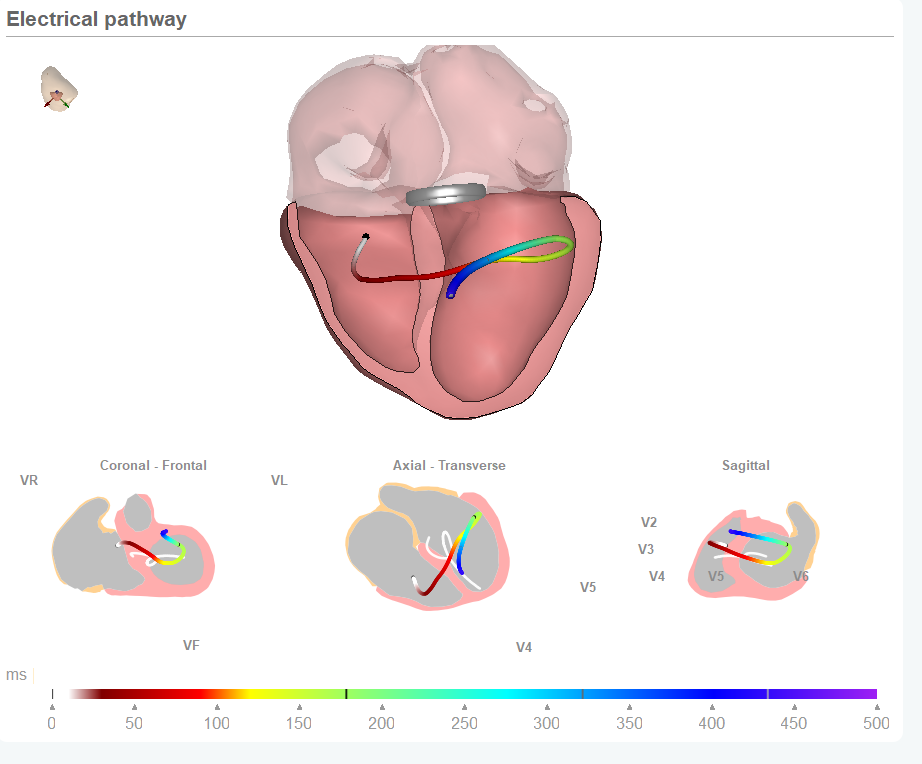
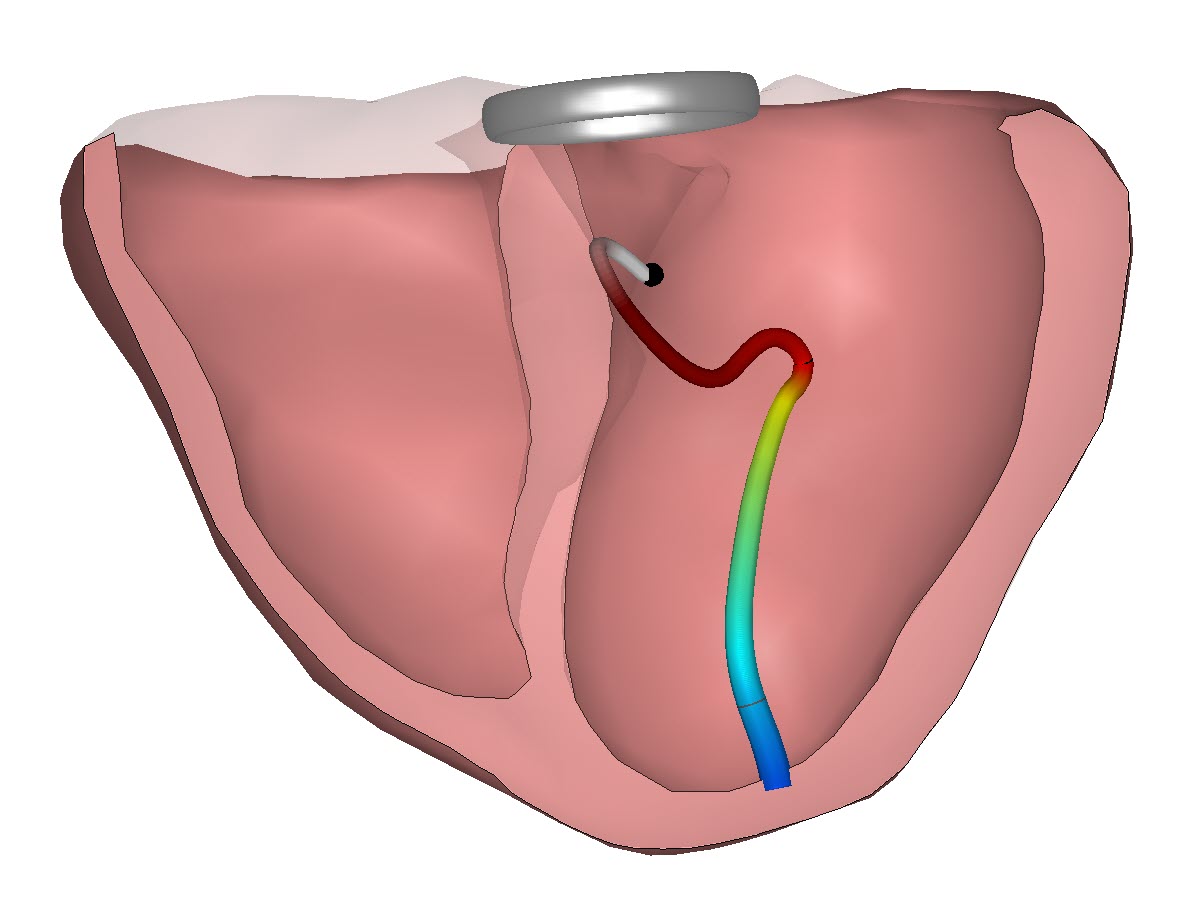
In this article the delta wave is introduced as an additional view on the heart performance. The delta wave compares the recorded ECG waveforms with a distribution of normal healthy persons waveforms.
In our CineECG application this difference is now part of the comparison and supports the increase of accuracy in identifying cardiac abnormalities.