The female heart is different. This wisdom is a growing factor in today’s cardiology practice. However, gender-related heart studies are scarce. Most focus is on the differences in characteristics when heart infarcts or other cardiovascular diseases become manifest and the challenge is to learn physicians to take a broader view on triage checklists. Key studies which been executed and published indicate significant differences between males and females in their response to diseases. In 2018 Adjei, Xue and Mandic investigated the differences in ECG response to stress. Their study showed differences in heart rate variability. And in several situations within the stress and heart activation cycle the male and female heart rate variability response is just opposite (increase versus decrease and vice versa). This study was a clear signal for physicians to not take the Male dominated date regarding response to stress as the ‘normal’.
In another study Mieszczanska and others demonstrated there are clear gender-related differences in ECG presentation and prognostic significance of ECG findings between males and females after a heart infarct has occurred. Their study showed a significant difference in the so-called ST segment of the activation and recovery cycle (when the heart starts to relax after the muscles have contracted). Again it is an opposite finding: for males look at ST depression and for females look at ST elevation. From our perspective another signal to use different ‘normals’ for males and females.
New gender differences in the ECG Normals.
These studies mainly focus on difference between males and females after a cardiac incident has occurred. And show the female heart is different in its response. But the female heart is different in its physiology as well. First, on average the female heart is somewhat smaller in size. But this does not really impact the normals on the level of heart rate or activation times in healthy people and being male or female is irrelevant. So far so good for heart rate and rhythm variables. But as seen in the second mentioned study the ECG waveforms are not evaluated in terms of quantitative parameters. Qualitative terms as depression, elevation, inverted are used to describe the recorded value. These assessments are based on the so-called base-line in the ECG which is derived from the earlier part of the activation cycle.
New ECG interpreation solution applies gender differences
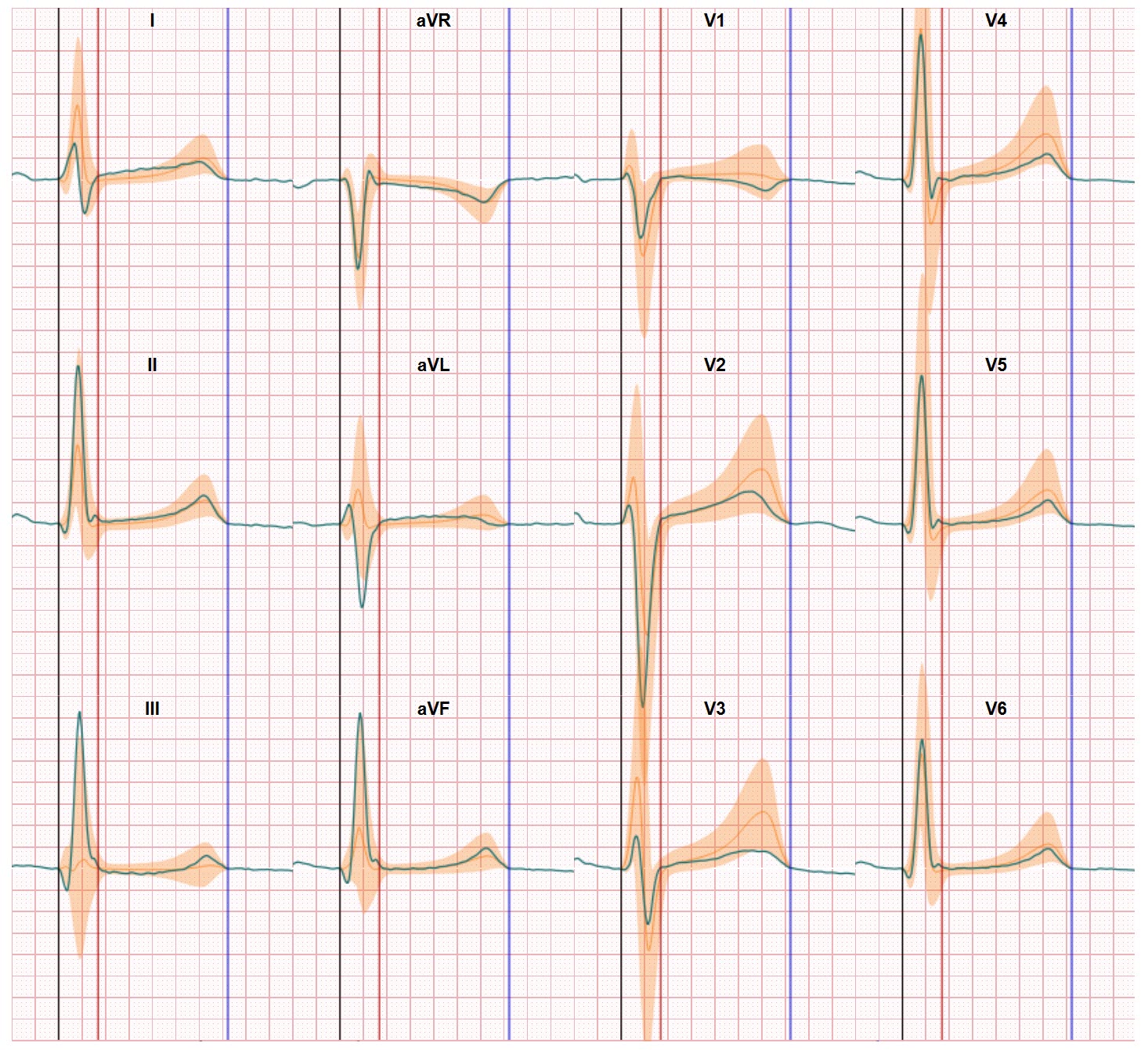
In developing our ECG interpretation solutions we take a new view on ECG normals and the normals of the ECG waveforms and their shapes and amplitudes. Our research has demonstrated there’s a significant difference in the normal for male and female ECG amplitudes. If you evaluate these waveforms on the regular print format it’s very hard to see for a physician who is used to make a visual assessment. But if you standardize the process and ECG results and create a normal distribution of normal amplitudes the differences in amplitudes between males and females are clear. The female heart is different. Also in this respect. And since the normals of females end up within the normal range of male ECG amplitudes the risk is apparent for not identifying abnormal heart performance within females. In our technology the gender-related differences are already embedded in our software. The female heart is different and this should be part of the standard triage process.