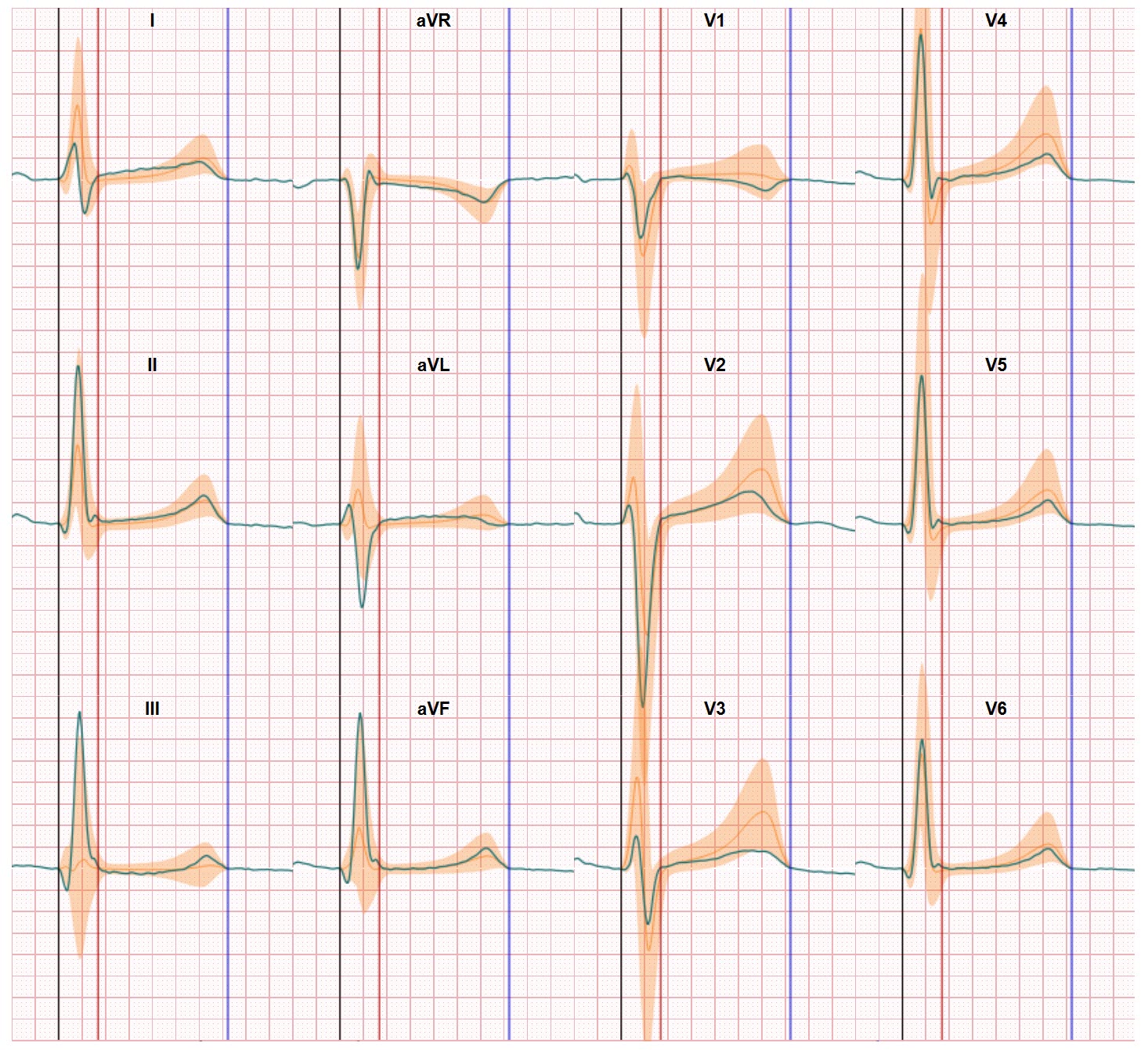
ECG electrode placement variability and differences in inter-individual human anatomies can lead to misinterpretation of ECG examination. Electrocardiography is nowadays one of the most widely used diagnostic methods in screening tests for early detection of cardiac diseases. Recording an ECG is noninvasive and may have a large impact on clinical diagnosis and on further medical treatment. The ECG signals reflect the electrical activity of the heart muscle as it is sensed by electrodes placed on the body surface. In clinical practice, the most commonly used electrodes layout is 12-lead standard ECG system.
One of the main sources of mistakes is inaccurate ECG electrode placement in suggested positions on the torso. Another main sources is not knowing the exact heart position in the torso. Both factors, dependent and independent on medical staff, can cause the change of the distance between the electrodes and source of the signal in the heart. And influence the angle on how the electrodes record the electrical activation. It’s like making an picture with your camera and move a bit aside to make another picture of the same object. These images than are each taken from a different angle and the image will be different. All these factors influence the graph of the ECG waveforms. As was described in an interesting article by Michal Kania and others in Medical & Biological Engineering and Computing.
The position of the ECG electrodes is especially critical for the electrodes placed closes to the heart. These electrodes are called pre-cordial electrodes. The positions of the electrodes placed on arms and legs are less influential on the ECG waveforms.
And, another important issue which should be taken into account is the variability of precordial lead placement in ECG recordings. Kerwin et al. [12] reported that correct lead positions with an error less than 1 cm of recommended positions were achieved by trained technicians only in case of 50 % of studied men and 20 % of studied women. They found that electrode placement error often was in the range of 2–3 cm, but occasionally reached even 6 cm. And although Kerwin focused on the reproducibility of ECG electrode positions the overall observation is the variability of ECG electrode positions and their influence on the ECG waveform.
Computerized modeling to solve the problem of ECG Electrode placement variability
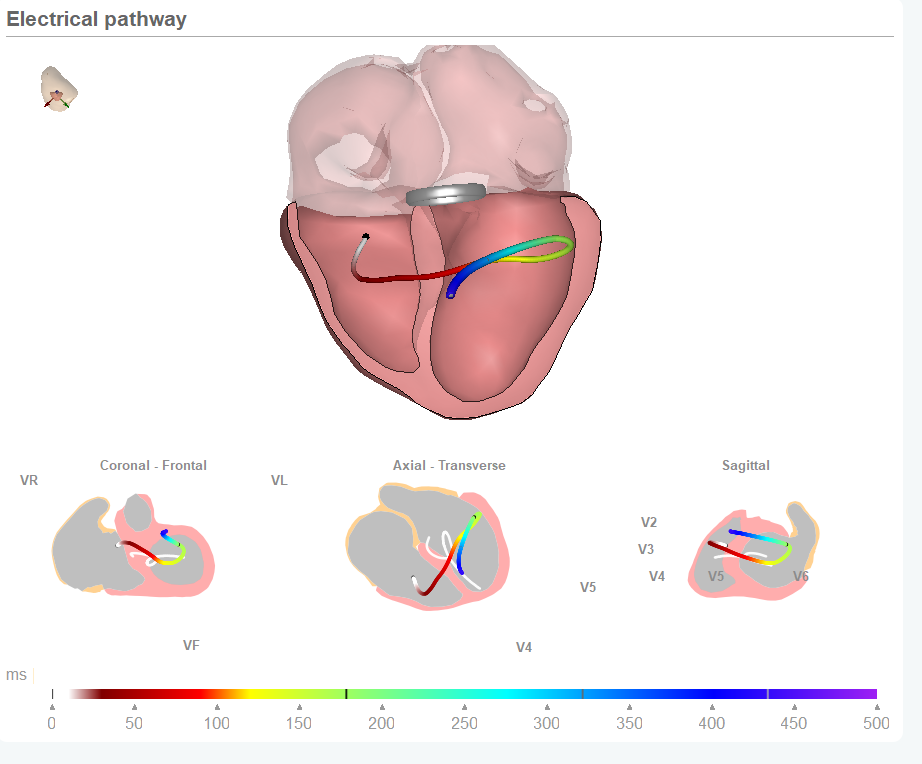
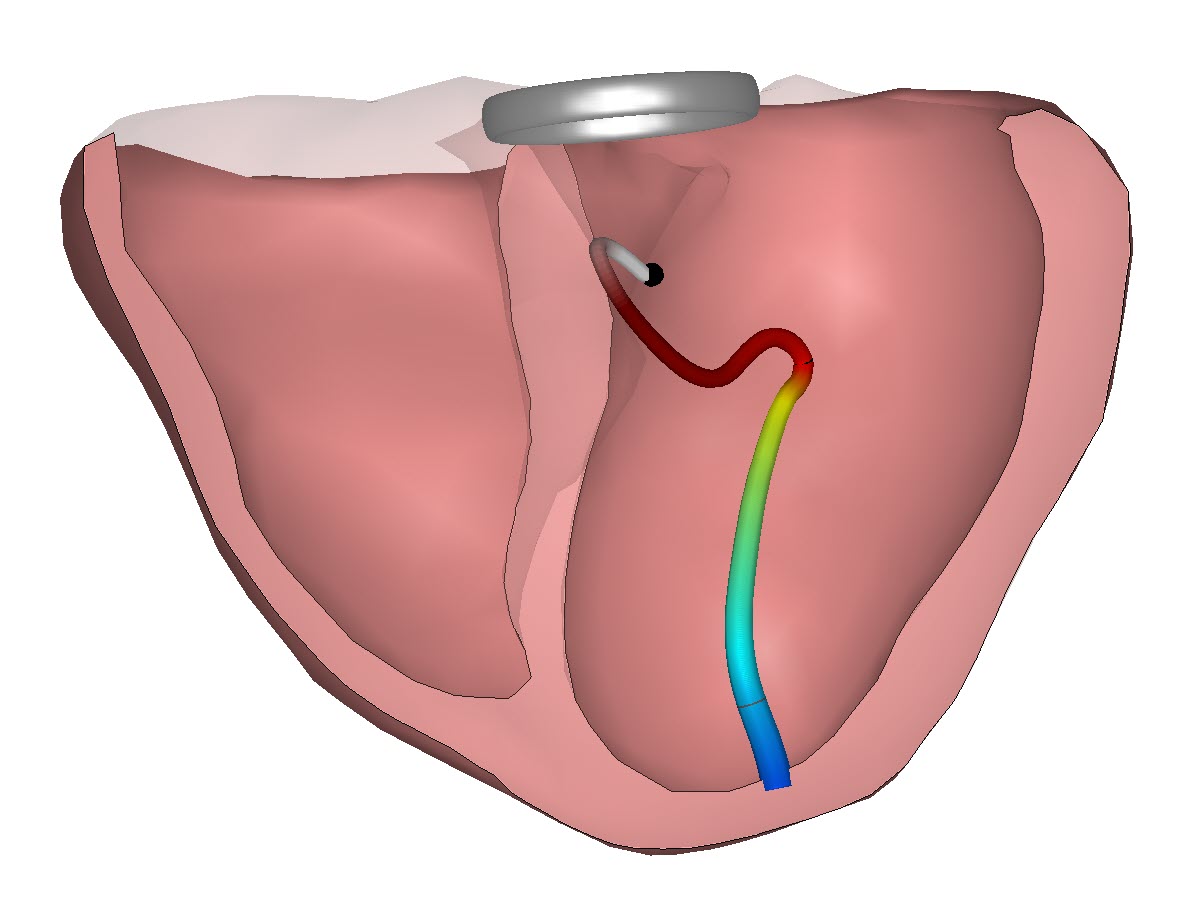
Over the years the issue of ECG electrode placement variability has not been addressed properly. Scientist even dreamed of tattooing as a solution to ensure correct replacements. But even that solution did not address the initial problem of doing it right first time. Today computerized modelling may offer a way forward. In this approach we use computerized models of the heart, its conduction system, the torso, the relationship between torso and heart and also of the ECG electrode positions.
If done properly we can reduce the impact of the actual ECG electrode positions and enable physicians to see more in the ECG. Within this approach the ECG data is related to the heart anatomy and this way the sensitivity of the heart activation mapping for ECG electrode placement variability is significant reduced especially in the parts of the heart activation with low potential differences such as the ST segment and the T wave. New options for improved ECG waveform interpretation are now turned into reality.